Pandemic likely catalyst for future deals and partnerships
![]()
Stay informed on the latest industry news, best practices, and trends in revenue cycle management for hospitals and physician groups.
![]()

![]()

![]()

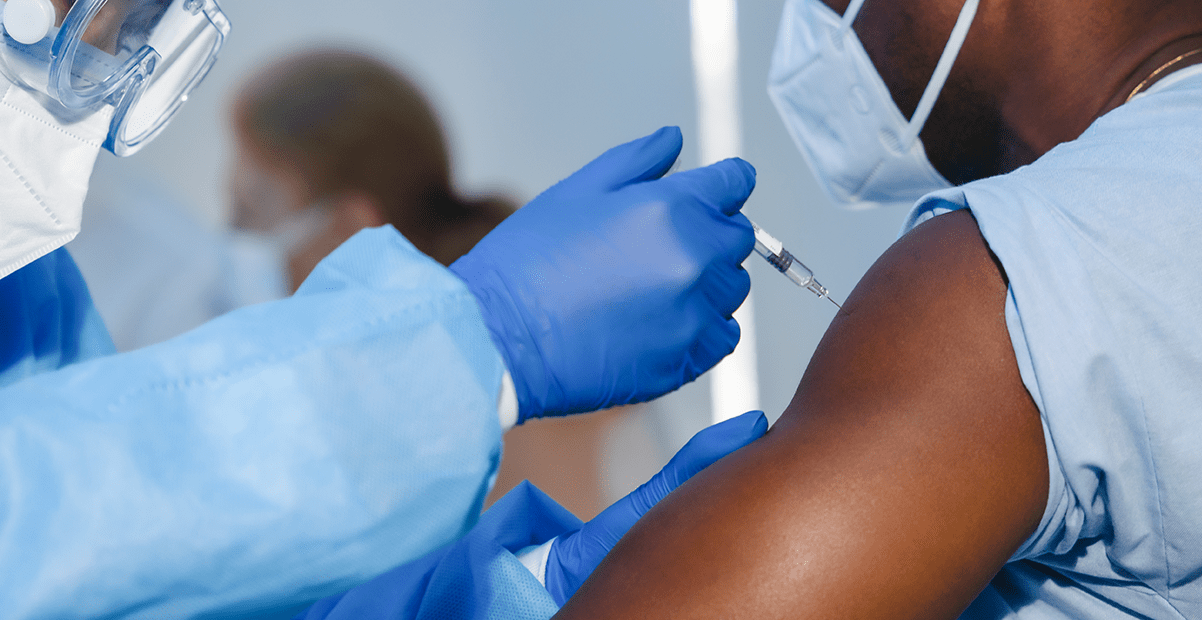
The American Hospital Association (AHA) was hoping for intervention from the D.C. Circuit Court of Appeals as the Price Transparency rule requiring hospitals to publicize rates goes into effect Friday, January 1, 2021. The AHA filed for an emergency notion to block the rule from going into effect, citing hospitals are overwhelmed with COVID-19 vaccine distribution and record-high caseloads of COVID-19.
![]()

Below are some of the key healthcare-related provisions in the legislation, including a detailed breakdown of the provisions related to funding for healthcare providers under the COVID-19 Provider Relief Fund (PRF).
![]()

The agency also released payment allowances for the two billing codes, which account for the injection, infusion, and post-administration monitoring of the recently approved COVID-19 antibody drug.
![]()

![]()
![]()
Ensure Compliance with CMS Payer Price Transparency Rules
Quickly deploy secure, compliant and user-friendly web pages where patients can interactively explore shoppable services and create personalized estimates.
![]()