Increase lab reimbursement with a Patient Access Management solution
![]()
Discover the latest news, trends, and best practices in revenue cycle management for lab and diagnostic providers, including coding, billing, and collections.
![]()

![]()

![]()
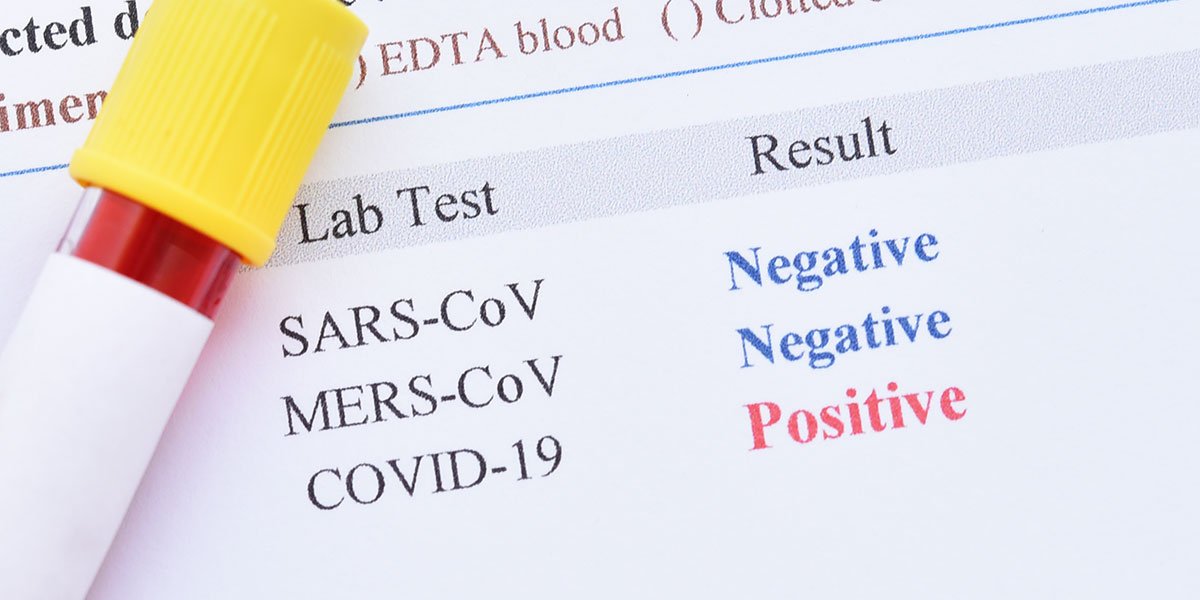
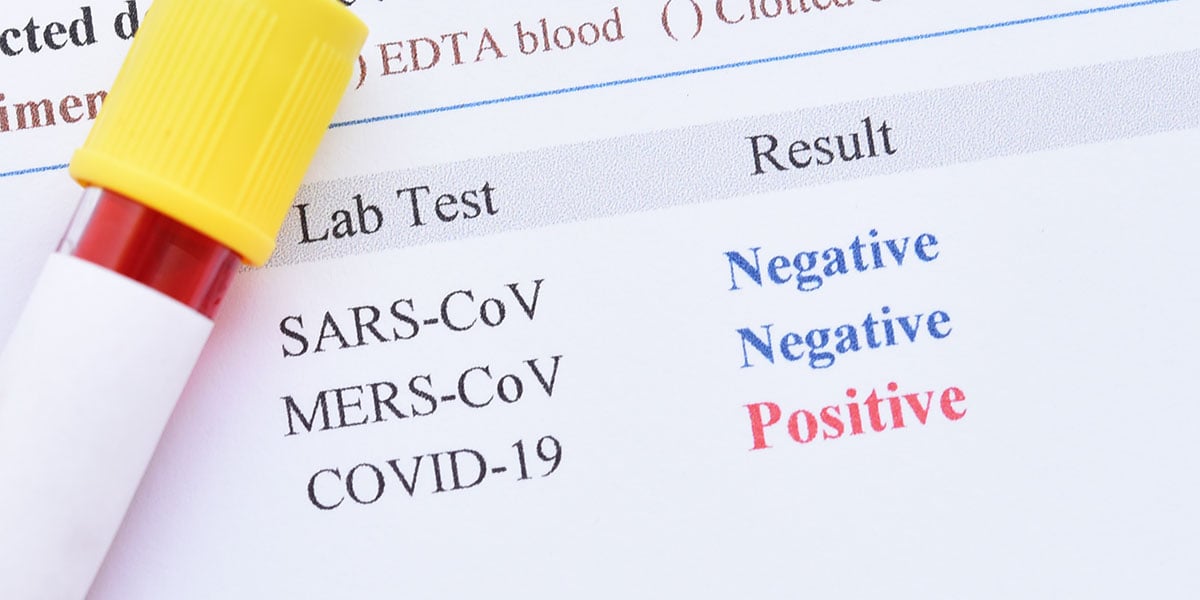
UnitedHealthcare (UHC) is making process changes to their Genetic and Molecular Lab Testing Program, effective June 1, 2021. These changes will impact the process for requesting prior authorization and registering lab tests. UHC stated that more details and training webinars will be provided before June 1, 2021.
Please note the following:
Changes to the prior authorization process
Changes to the lab test registration process
For more information please visit Genetic and molecular lab testing program changes – Frequently asked questions – UnitedHealthcare.
Source: https://www.uhcprovider.com

![]()

![]()
“By outsourcing our billing to Quadax, we were able to focus on our clinical mission—helping providers offer a personalized approach to cancer care for patients facing lung cancer.”
For its lab tests, Biodesix found that payers often required validation in the form of prior authorization, medical records and more—but often after the claim had been submitted. They sought a better way.
Biodesix partnered with Quadax and working collaboratively, developed a custom database specific to Biodesix, utilizing payer information from over 800 payers and designing workflows specific to their needs. The result? Fewer denials and greater efficiency.
![]()

![]()
![]()