

By definition, consumerism is a social and economic order that encourages the acquisition of goods and services in ever-increasing amounts. Continue reading “A New Era of Consumerism Facing Labs Today – How Do You Stay Competitive?”
Category: For Laboratories
Discover the latest news, trends, and best practices in revenue cycle management for lab and diagnostic providers, including coding, billing, and collections.
Is Your Lab Collecting What It’s Owed?

With so much of healthcare reimbursement administered by contracts, expected net patient service revenue is often a function of the payment terms and conditions found in payer-provider contracts. In order to identify underpayments, wrongful denials and shortfalls, labs need an effective, automated contract management solution as part of their A/R processes.
Why Contract Management?
Regardless of laboratory type or size, every lab can benefit from automating the validation of every single claim against the contracted amount. A proper contract management solution helps to increase a laboratory’s revenue by identifying every dollar that should have been paid per provider contracts, supplying data for contract negotiations, powering accurate revenue forecasting, and decreasing manual work hours dealing with contracts; all while automating underpayments and denials to help achieve 100% collectability.
5 Tips to Help Plug Revenue Leaks
-
- Utilize contract modeling to build all net patient service revenue contracts, provider-to-client invoice-based contracts, all payment terms and conditions, for multiple years, including:
• Medicare/Medicaid schedules
• Government, third-party payer and client billing fee schedules
• Fee schedules for non-contracted payers
• Percent of charges
• Percent of Medicare
• Carve outs
• Outliers
-
- Create and maintain an actionable workflow to help pursue priority claims during pre-billing based on expected revenue versus total charge. Be sure to define payment variance rules and apply post adjudication to determine next steps.
- Validate charges to prevent charge master errors before a claim is submitted by configuring non-contracted payer rules to validate acceptance of patient co-insurance.
- Take advantage of cash flow analytics and variance reporting to calculate cash flow by payer, age of claim, and where the claim is in the revenue cycle. This analysis and reporting will help identify opportunities for maximum cash flow improvements in the revenue cycle. Variance reporting specifically will provide an immediate indicator of adjudication outside contracted rates.
- Simplify the collection and revenue recovery process by identifying underpayments to trigger automated appeal process.
Plug your revenue leaks by identifying and collecting on underpayments and wrongful denials by being armed with the correct contractual data to appeal and overturn them. Contact us today to learn how Quadax can help you collect what your lab is owed!
Surprise Billing Legislation: Ways to Mitigate Your Risk

Nearly 60% of insured adults have received a surprise bill on a healthcare service they thought was covered by insurance. And whether care or the provider is in-network, out-of-network or a mix of the two, 1 in 5 of these insured adults find it difficult to pay their deductibles.2 Why is this happening and what is being done about it?
Due in part to narrow provider networks, surprise bills can be the financial result of a patient receiving in-network care by an out-of-network provider, often the bill being the difference between the charged and the allowed amount of a service. These surprise bills can cause undue stress and have detrimental financial effects on the entire household, such as delayed payment on other household expenses, mounting credit card debt, and more. As such, state and federal legislations are responding in kind with laws around surprise bills.
STATE LEGISLATION
A number of states have enacted comprehensive laws to protect some patients from surprise medical bills, including California, Oregon, Illinois, Florida, New York, New Hampshire, New Jersey, Connecticut and Maryland. Additional states, including Texas, Colorado, New Mexico, and Washington, have passed laws expected to take effect this year. In essence, these laws are meant to protect consumers from surprise bills by limiting providers to the applicable in-network cost, setting a state payment standard, and/or establishing a dispute resolution process.3 Meanwhile, more than a dozen more states have enacted a limited approach to mitigate surprise bills.
FEDERAL LEGISLATION
Federal action is necessary to address certain aspects of surprise bills for people enrolled in self-funded plans due to the Employee Retirement Income Security Act of 1974, or ERISA. Legislation is expected to be passed in fall of 2019.
Both state and federal initiatives can be summed up as:
- All proposed legislation includes a ban on balance billing patients
- Most legislation is specific to emergency and ancillary providers at this time
- Many of the proposed state and federal bills include stipulations for using usual and customary rates as a basis for negotiation
- Arbitration clauses included in many of the proposed bills is considered favorable to providers
- Indexing against usual and customary rates seems to be included in more of the state initiatives
What can you do?
To help avoid and mitigate the risk of surprise bills, more and more hospitals and clinical laboratories are rethinking the patient experience and investing in tools to help provide pricing transparency on procedures and services, like testing. These tools utilize basic patient demographics (name, birthdate, address, insurance provider, etc.) to validate insurance coverage and eligibility, perform advanced benefit investigation to uncover plan-specific coverage details, assess prior authorization rules, and most importantly provide a patient’s expected out-of-pocket cost. Taking it even further, labs can identify a patient’s propensity and willingness to pay to help assess the need to offer financial assistance. This entire approach, called Patient Access Management, can help clinical labs and providers alike offer the transparency needed to empower a patient to make financial decisions regarding their care – perhaps the patient cannot afford the test so an alternative treatment plan has to be put into place. Patient Access helps to improve the patient experience in that the patient understands exactly what they will owe for the test – and no surprise bills. For a growing molecular lab, this can mean the difference between writing off bad debt and securing expected revenue.
To learn more about Patient Access Management solutions offered by Quadax and how they can help mitigate the risks of surprise bills and more, contact us today!
- http://www.norc.org/NewsEventsPublications/PressReleases/Pages/new-survey-reveals-57-percent-of-americans-have-been-surprised-by-a-medical-bill.aspx
- https://www.consolidatedcredit.org/infographics/medical-debt/#gref
- https://www.healthsystemtracker.org/brief/an-examination-of-surprise-medical-bills-and-proposals-to-protect-consumers-from-them/#
MIPS Scoring for Facility-based Pathologists: 3 Things You Need to Know

There are two pathways under the Quality Payment Program (QPP): MIPs and Advanced APMs. Unless you qualify as a participating clinician in an Advanced Alternative Performing Model, MIPS will be your default. MIPS has four weighted performance categories, identified below. This post will focus on Quality and Cost.
- Quality
- Improvement Activities
- Promoting Interoperability
- Cost
As a facility administrator, navigating the requirements to be successfully compliant with MIPS can be confusing, especially for those CMS considers non-patient facing clinicians, like pathologists. Pathologists must optimize their participation in order to minimize the risk of losing out on bonus opportunities stemming from new and evolving CMS payment models. One of those models centers on the new policies of Facility-Based Measurements. As a facility administrator, what do you need to know?
1. Definition of facility-based
Individual Facility-based clinician
• Must have 75% or more of covered professional services in any of the following:
◽ Inpatient hospital (POS 21), or
◽ On-campus outpatient hospital (POS 22), or
◽ Emergency room (POS 23), and
◽ Have at least one service billed with POS 21 or POS 23
Facility-based group
• At least 75% of MIPS-eligible clinicians billing under the group’s TIN are identified as facility-based.
Attributed to a facility with a Hospital VBP score
2. Your facility-based status
The easiest way to determine and confirm your 2019 Facility-based status is to start with CMS by utilizing their online MIPS eligibility and look-up tool, found at https://qpp.cms.gov/participation-lookup. (You will need your HCQIS Access Roles and Profile System (HARP) credentials, Tax Identification Number (TIN) and National Provider Number (NPI).) This tool will also inform you if you are exempt from MIPS, in which case, you will not be responsible for MIPS reporting. If you are not exempt, the tool will provide you with any special status needed for reporting other than facility-based. The tool will also indicate your attributed facility if you have facility-based status.
If you are a facility-based pathologist or group, CMS will automatically assign you Quality and Cost scores for based on the attributed facility’s Hospital Value-Based Purchasing (HVP) program. CMS will assign these scores even if you are not a patient-facing clinician.
Facility-based pathologists should attest to Interoperability Activity scores separately to maximize their MIPS score. Facility-based pathology groups must attest to these scores separately from the facility in order to be assesses as a group and to maximize their MIPA score.
3. Your potential 2019 MIPS performance
You can preview your Quality and Cost scores on the QPP website for estimated 2019 MIPS performance period, based on 2019 Hospital VBP Total Performance Scores (TPS) mapped to 2017 performance QPP data.
The 2019 MIPs scores will use 2020 Hospital VBP scores mapped to QPP data from the 2019 performance period. Note, scores between the preview and 2019 MIPS may change. How? There could be changes in the hospital to which the clinician or group is attributed. There could be updates to the HVBP TPS between 2019 and 2020 at the attributed hospital. Or, there could be updates to the distribution of MIPS quality and cost performance scores. The College of American Pathology suggests you may want to report on MIPS separately if you are not confident in your hospital’s VBP score as CMS will take the higher score from your reporting data.
The CMS recommends that eligible professionals check with the QPP Help Desk for more information on measures and the QPP.
QPP Help Desk Contact Information:
7:00 AM–7:00 PM CT Monday – Friday
email: QPP@cms.hhs.gov
Phone: 866-288-8292
*Adapted from Facility-Based Measurement: A Practical Overview, by Emily E. Volk, MD, MBA, FCAP (Aug 2019).
Seven Keys to Improve Out-of-Network Collections
Reimbursement in out-of-network care has grown to $60B and continues to grow due to the proliferation of narrow networks. Many providers don’t play in the out-of-network space or write-off a big chunk of revenue to close out an aging A/R. So what does an organization need to do in order to maximize reimbursement in this arena?
According to Richa Singh of Collection Rx, 5-10% of healthcare revenue is lost due to lack of time and technology associated with the work involved to follow up on the cost of collections resulting from unprocessed claims, missing documents, and denials. In many instances, providers overlook claims that are not properly processed and, as such, miss out on revenue. More importantly, almost 40% of that revenue loss is in individual out-of-network claims, mostly due to inexperience with these types of claims as a result of no data with the payers and no time or staff to commit to understanding their rules let alone track down the revenue.
Many providers don’t play in the out-of-network space or write-off a big chunk of revenue to close out an aging A/R. Yet with so many stringent rules for in-network, the biggest revenue growth opportunity exists in out-of-network care! So what does an organization need to do in order to maximize reimbursement in this arena?
1. Understand Payer Tactics
Payers, unfortunately, have cost containment practices on what they consider unnecessary tests or treatments. When these services or payment are not contracted or clearly understood, providers miss out. You need to:
• Know a payer’s out-of-network payment trends and policies
• Have access to the data to prove a payer’s inadequate reimbursement
• Be persistent
• Dedicate the right resources with your efforts
Getting ahead of these roadblocks with technology to support your efforts of clean claims, maintain proper documentation, provide medical necessity, show submission of claims, and decipher EOBs will help increase out-of-network reimbursement.
2. Invest in Technology
Data and automated workflow rules will help improve your overall reimbursement rates and ensure you get paid for your services. Areas of suggestion include:
Workflow – Automate manual processes as much as possible
Data – Analyze data and comparable claims to understand payer trends
Coding – Supports workflow optimization to lower collection costs
Analytics – Deep dive into your metrics for strategic planning
3. Maintain In-depth Reconciliation Process Through Collections
Avoid missed revenue with automated workflow and checks and balances throughout the collection process.
4. Streamline Your Workflow
Identify weak links in the front-end of your A/R to avoid issues on the back-end, improving staff time management and reducing the cost to collect.
5. Gain Expertise in Out-of-Network Benefits/Payments
Drive business decisions by having access to actionable data that will allow analysis, such as root cause identification on underpayments and denials, and help identify trends, projections, and revenue impact on a weekly, monthly and even ad hoc basis to help improve financial performance.
6. Gain Out-of-Network Expertise
With a growing market of unrestricted contracts in out-of-network, there is an untapped opportunity to increase reimbursement rates and impact your bottom line. You need to know the trends and tendencies of out-of-network payments, have comparable data to counter tactics, and understand those tactics.
7. Outsource Payer Collection Efforts
Ensure your partner is provider-centric in that it is providing access to your collection data, helping you with reporting and understanding metrics of importance, and offering frequent success and troubleshooting reviews.
8. Enhance Patient Experience
Pricing transparency has been shown to improve collection efforts for self-pay patients. When a patient is aware of their financial expectations sooner, labs and the ordering physicians can avoid the run-around that often results from “surprise bills.”
Quadax specializes in helping healthcare providers maximize reimbursement – both in- and out- of-network – through billing and software solutions geared to solve the challenges associated with navigating the payer landscape to help expedite claims and payment processing. Want to learn more? Let’s talk!
Content adapted from Strategies for Success in Out-of-Network and Payer Reimbursement, May 2019.
https://www.beckershospitalreview.com
Is Your Lab Applicable Under the New PAMA Definition?

PAMA has already made a significant impact for hospital and independent labs, and continues to do so with the redefinition of an applicable lab. PAMA has expanded the number of reporting labs to include smaller labs and hospital outreach labs. CMS estimates at least 43% more labs are now required to report under the new definition. Therefore, labs not reporting during the first period need to double check their requirement.
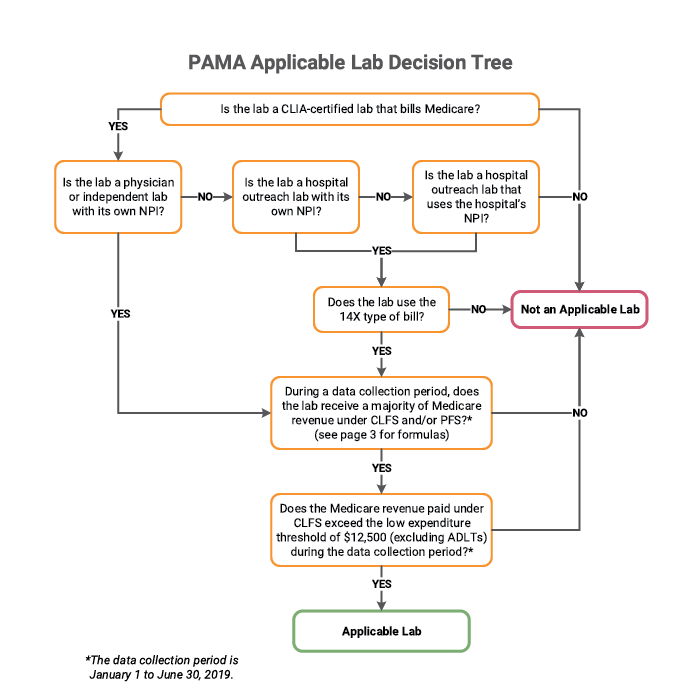
As defined by CMS, an applicable lab is a laboratory receiving more than 50% of its total Medicare revenues from services paid under the CLFS or the physician fee schedule (PFS), with a low expenditure threshold. To meet the low expenditure threshold, a lab must have received $12,500 from final Medicare paid claims for services paid under the CLFS during the data collection period of January 1 to June 30, 2019.
A new wrinkle per the 2019 Final Rule is that Medicare Advantage revenues are excluded from the total Medicare revenue calculation. The change for round 2 that may have the greatest impact is that hospital outreach laboratories billing “non-patients” for laboratory services are now included in the applicable lab determination.
In Transmittal 3425, a non-patient is defined as a beneficiary who has a specimen that is submitted to a hospital for analysis but is not physically present at the hospital for the laboratory service; that is, the patient is neither a registered hospital outpatient nor an admitted hospital inpatient. Non-patients may be identified with the CMS-1450 14X TOB. An inherent challenge is that the 14X bill type is not necessarily used by commercial payers. This seemingly small modification will have significant impact to which organizations are considered “applicable labs” and to the algorithms by which providers select data for reporting.
Labs meeting these qualifications must then report “applicable information” to CMS. As a service to our clients, Quadax has developed the PAMA Applicable Lab Decision Tree shown below, which visually depicts the determination criteria.
Quadax financial reporting quickly and accurately provides the data needed to walk through this process and determine a lab’s status under PAMA. Quadax supports laboratories with tools to meet all regulatory requirements touching the revenue cycle. In addition to equipping labs with tools to help them identify their PAMA applicable lab status, Quadax makes it easy for applicable labs to select and segregate the correct, complete data required for submission.
To learn more, join us during this complimentary webinar, PAMA Tools & Strategies for The Next Round of Reporting on June 26, 2019 at 11:00 AM EDT.
This webinar will provide further insight into the strategies and tools successful labs use to determine applicable lab status, capture the appropriate claims population, and supply and normalize data to meet PAMA Reporting guidelines.
Patient Access Antidote: Retaining More Revenue with Front End Solutions
Take a deep dive into consumer trends impacting the revenue cycle of clinical labs and best practices in patient access management.
Patient Access Antidote: How Labs Can Retain More Revenue

Patients’ financial liability in paying for healthcare services is almost unrecognizable from that prior to the early 2000s; yet many organizations, including clinical laboratories, have struggled to modernize their collection practices in turn. As a result of this mismatch, labs risk not just losing out on uncollected revenue, but also wasting time and resources on futile or minimally effective back-end collection efforts.
Reversing the problem is possible, however, by implementing the right best practices and revenue cycle management technologies. In particular, maximizing patient access early in the revenue cycle can help patients manage their financial responsibility and preempt many unnecessary denials, payment delays, and uncollected balances.
In this Dark Daily white paper – Patient Access Antidote: Retaining More Revenue with Front-End Solutions – take a deeper dive into the consumer trends having an impact on revenue cycle management, best practices in patient access management, and the expert-recommended tools and solutions that clinical laboratories can employ to respond.
We are also presenting on Patient Access topics at the 24th Annual Executive War College. If you are attending, don’t miss these opportunities to learn new strategies to help your lab sustain financial stability and growth. {Quadax is proud to be a Benefactor Sponsor of this annual conference.}
| Tuesday, April 30 | 8:30 a.m. | Brean Bark Director, Product Development |
| Missy Tubbs Senior Product Manager |
|
| Patient Responsibility & Payer Pre Billing Requirement Impacting Your Bottom Line? Engage Physicians and Patients with Patient Access Solutions & Analytics To Improve Revenue. |
|
| Wednesday, May 1 | 7:30 a.m. | Walt Williams Director of Revenue Optimization and Strategy |
| Are Your Patients Now Your Payers? New Tools Empowering Your Lab to Collect More Money, Faster, and at Less Cost.
|
|
At Quadax we take on your billing needs so you can do more to improve the delivery of value-based care and transform patient outcomes. Explore our revenue cycle optimization solutions to expedite payment, maximize reimbursement, and enhance visibility into your business. Get in touch with our RCO team and discover how we can help you create areas of opportunity to achieve the best possible revenue outcome.
Pursue LDT Revenue Cycle Success with Cross-functional Collaboration

In many traditional lab organizations, the scientific product development group has historically produced new diagnostic tests without meaningful input and consideration of payer policy and revenue cycle demands. But what if the lab were to begin considering the needs of the revenue cycle even earlier? What if revenue cycle considerations were included in the lab’s decision-making about test development and commercialization? How could collaboration between the lab and its revenue cycle group help improve financial performance? Labs who integrate revenue cycle management considerations into new test development have a higher chance of reimbursement success and achieving profitability.
Bringing the revenue cycle and the lab together.
Labs who consider revenue cycle issues at all stages from the beginning of the test development through deployment and billing, are able to gain synergies and successfully implement a cohesive commercialization strategy. Collaboration between sales, marketing, laboratory personnel, and other stakeholders is key, especially for lab’s developing and launching novel diagnostic tests. When information flows both ways, the development team provides the necessary information to help the financial team make revenue and volume forecasts that are more realistic. Conversely, feedback to the lab that considers the existing medical payer policy environment, clinical utility guidelines, and revenue cycle demands can potentially lead to development of more commercially viable tests.
How the lab benefits from collaboration.
Scientific advisors of the laboratory have expertise in a molecular testing technology, modality, or other unmet healthcare needs that would lend itself to development of a new test. Many laboratories spend their R&D budget on new assay development without fully understanding the reimbursement environment for the test they are developing. Early revenue projections may be overly optimistic, and may not account for limited payer coverage for the test.
A new test that may prove “popular” with clinicians may bring in a large volume of business, but if reimbursement rates are low or result in greater patient cost-share, the financials of that test may not be beneficial to the lab. The ability to identify which tests, patient populations, providers, and payers perform best financially, and which do not, can help guide the laboratory in test development decisions. With a cross-functional team—commercial, marketing, revenue cycle, finance, and payer relations/market access—input from both lab management and those responsible for financial operations can influence R&D direction.
How the revenue cycle benefits from collaboration.
Marketing and sales teams must differentiate a lab’s new test from other treatment options, so that physicians will deem it clinically necessary for their patients. Communications need to be developed to inform physicians, patients, and payers as to the use and benefits of the new test.
When the lab comes together with its revenue cycle during test development, the cross-functional team can methodically address the following questions and capture the necessary data needed for commercialization communications. If the payer will not pay for the test, what evidence must be developed to secure positive coverage and what is the timeline for developing such evidence? What is the marketing message and will it need to include specific intended use guidelines? What pre-test requirements (e.g. medical policies, prior authorization) will exist for the test? What is the appeal strategy? What is the patient billing strategy? What is the institutional/client billing strategy?
When cross-functional collaboration is limited or lacking, what are the associated risks?
If different teams within a lab are not collaborating, the unintended consequences can be high costs and minimal revenue. Demonstrating clinical relevance can suffer, and insurance companies may choose to either not cover the test or cover it with many restrictions and with sub-optimal reimbursement.
When collaboration is lacking or limited, objectives within the lab may become misaligned. Sales might offer resistance to billing and finance, trying to balance gaining market traction and order volume against accepting samples that may not meet the clinical criteria for reimbursement. Investors and senior management may focus too early on driving revenue, versus evidence development. In its pursuit of growth and volume, the laboratory’s organization may hire a large sales team to drive utilization well before the evidence is ready to support broad coverage and reimbursement.
Building cross-functional collaboration to manage these risks.
What are the challenges a lab will face when bringing new diagnostic tests to market and what can a lab do to circumvent these challenges to achieve its financial goals? View our Cross-functional Collaboration Is Key to Diagnostic Test Commercialization whitepaper to learn more about what your laboratory can do to make your LDT a revenue cycle success.
Quadax understands the issues and industry challenges facing your lab today. We partner with our clients to provide a complete revenue cycle solution—with expertise focused on patient access; claims, reimbursement, denials and appeals management; and business analytics we offer a lab-centric revenue cycle solution. To learn more about how Quadax can help, view our revenue cycle optimization solutions.
Cross-functional Collaboration is Key to Diagnostic Test Commercialization
This white paper is to help organizations that provide and develop diagnostic lab tests understand the need for strong cross-functional collaboration between the revenue cycle and the lab prior to commercialization.